VO2 Max, Aerobic Power</ br>& Maximal Oxygen Uptake
VO2 max has been defined as:
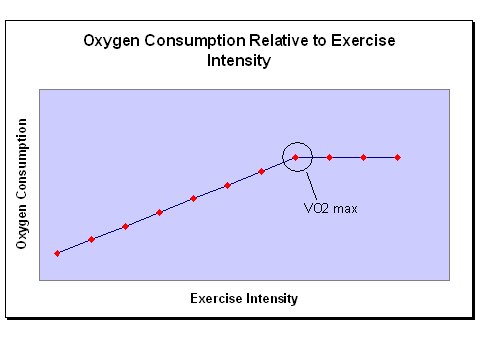
The point at which oxygen consumption plateaus defines the VO2 max or an individual's maximal aerobic capacity. It is generally considered the best indicator of cardiorespiratory endurance and aerobic fitness. However, as well discuss in a moment, it is more useful as an indicator of a person's aerobic potential or upper limit than as a predictor of success in endurance events.
Aerobic power, aerobic capacity and maximal oxygen uptake are all terms used interchangeably with VO2 max.
VO2 max is usually expressed relative to bodyweight because oxygen and energy needs differ relative to size. It can also be expressed relative to body surface area and this may be a more accurate when comparing children and oxygen uptake between sexes.

One study followed a group of 12-year-old boys through to the age of 20 - half of which were trained, the other half untrained but active. Relative to bodyweight no differences in VO2 max were found between the groups suggesting that training had no influence on maximal oxygen uptake. However, when VO2 max was expressed relative to body surface area, there was a significant difference between groups and maximal oxygen uptake did indeed increase in proportion to training (4).
VO2 Max In Athletes and Non Athletes
VO2 max varies greatly between individuals and even between elite athletes that compete in the same sport. The table below lists normative data for VO2 max in various population groups:

Genetics plays a major role in a persons VO2 max (11) and heredity can account for up to 25-50% of the variance seen between individuals. The highest ever recorded VO2 max is 94 ml/kg/min in men and 77 ml/kg/min in women. Both were cross-country skiers (16).
Untrained girls and women typically have a maximal oxygen uptake 20-25% lower than untrained men. However, when comparing elite athletes, the gap tends to close to about 10% (3). Taking it step further, if VO2 max is adjusted to account for fat free mass in elite male and female athletes, the differences disappear in some studies. Cureton and Collins (29) suggest that sex-specific essential fat stores account for the majority of metabolic differences in running between men and women.
Training & VO2 Max
Amongst groups of people following the same training protocol there will be responders - those who make large gains, and non-responders - those who make little or no gains (14,9). This was originally put down to a simple issue of compliance but more recent research suggests that genetics plays a role in how well any one individual responds to an endurance training program (13).
The extent by which VO2 max can change with training also depends on the starting point. The fitter an individual is to begin with, the less potential there is for an increase and most elite athletes hit this peak early in their career. There also seems to be a genetic upper limit beyond which, further increases in either intensity or volume have no effect on aerobic power (5). This upper limit is thought to be reached within 8 to 18 months (3).
Crucially, once a plateau in VO2 max has been reached further improvements in performance are still seen with training. This is because the athlete is able to perform at a higher percentage of their VO2 max for prolonged periods (2). Two major reasons for this are improvements in anaerobic threshold and running economy.
Resistance training and intense 'burst-type' anaerobic training have little effect on VO2 max. Any improvements that do occur are usually small and in subjects who had a low level of fitness to begin with (17). Resistance training alone does not increase VO2 max (30,31,32) even when short rest intervals are used between sets and exercises (33).
Considerable training is required to reach the upper limit for VO2 max. However, much less is required to maintain it. In fact peak aerobic power can be maintained even when training is decreased by two thirds (18). Runners and swimmers have reduced training volume by 60% for a period of 15-21 days prior to competition (a technique known as tapering) with no loss in VO2 max (19,20,21).
VO2 Max as a Predictor of Performance
In elite athletes, VO2 max is not a good predictor of performance. The winner of a marathon race for example, cannot be predicted from maximal oxygen uptake (15).
Perhaps more significant than VO2 max is the speed at which an athlete can run, bike or swim at VO2 max.
Two athletes may have the same level of aerobic power but one may reach their VO2 max at a running speed of 20 km/hr and the other at 22 km/hr.
While a high VO2 max may be a prerequisite for performance in endurance events at the highest level, other markers such as lactate threshold are more predictive of performance (3). Again, the speed at lactate threshold is more significant than the actual value itself.
Think of VO2 max as an athletes aerobic potential and the lactate threshold as the marker for how much of that potential they are tapping.
Factors Affecting VO2 Max
There are many physiological factors that combine to determine VO2 max but which of these are most important? Two theories have been proposed:
Utilization Theory
This theory maintains that aerobic capacity is limited by lack of sufficient oxidative enzymes within the cell's mitochondria (3). It is the body's ability to utilize the available oxygen that determines aerobic capacity.
Proponents of this theory point to numerous studies that show oxidative enzymes and the number and size of
mitochondria increase with training. This is coupled with increased differences between arterial and venous blood oxygen concentrations (a-vO2 difference) accounting for improved oxygen utilization and hence improved VO2max.
Presentation Theory
Presentation theory suggests that aerobic capacity is limited not predominantly by utilization, but by the ability of the cardiovascular system to deliver oxygen to active tissues. Proponents of this theory maintain that an increase in blood volume, maximal cardiac output (due to increased stroke volume) and better perfusion of blood into the muscles account for the changes in VO2max with training.
So what plays the greater role in determining an athlete's VO2 max - their body's ability to utilize oxygen or supply oxygen to the active tissues?
In a review of the literature, Saltin and Rowell (7) concluded that it is oxygen supply that is the major limiter to endurance performance. Studies have shown only a weak relationship between an increase in oxidative enzymes and an increase in VO2 max (8,9,10). One of these studies measured the effects of a 6-month swim training program on aerobic function. While oxidative enzymes continued to increase until the end, there was no change in VO2 max in the final 6 weeks of the program (10).
Determining VO2 Max
One of the most common is the Bruce protocol often used for testing VO2 max in athletes or for signs of coronary heart disease in high risk individuals.
Indirect testing is much more widely used by coaches as it requires little or no expensive equipment. There are many indirect tests used to estimate VO2 max. Some are more reliable and accurate than others but none are as accurate as direct testing. Examples include the multistage shuttle run (bleep test), 12 minute walk test and 1.5 mile run. Click here for some sample endurance tests used to estimate VO2 max in the field.
VO2 Max at Altitude
VO2 max decreases as altitude increases above 1600m (5249ft) or about the altitude of Denver, Colorado. For every 1000m (3281ft) above that, maximal oxygen uptake decreases further by approximately 8-11% (3). Anyone with a VO2 max lower than 50 ml/kg/min would struggle to survive at the summit of Everest without supplemental oxygen.
The decrease is mainly due to a decrease in maximal cardiac output. Recall that cardiac output is the product of heart rate and stroke volume. Stoke volume decreases due to the immediate decrease in blood plasma volume. Maximal heart rate may also decrease and the net effect is that less oxygen is "pushed" from the blood into the muscles (2).
Click here for more information on acclimatization to altitude.
Effects of Aging on VO2 Max
VO2 max decreases with age. The average rate of decline is generally accepted to be about 1% per year or 10% per decade after the age of 25. One large cross sectional study found the average decrease was 0.46 ml/kg/min per year in men (1.2%) and 0.54 ml/kg/min in women (1.7%) (22,23).
However, this deterioration is not necessarily due to the aging process. In some cases the decease may be purely a reflection of increased body weight with no change in absolute values for ventilation of oxygen. Recall, that VO2 max is usually expressed relative to body weight. If this increases, as tends to happen with age, and aerobic fitness stays the same then VO2 max measured in ml/kg/min will decrease.
Usually, the decline in age-related VO2 max can be accounted for by a reduction in maximum heart rate, maximal stoke volume and maximal a-vO2 difference i.e. the difference between oxygen concentration arterial blood and venus blood (2).
Can training have an affect on this age-related decline?
Vigorous training at a younger age does not seem to prevent the fall in VO2 max if training is ceased altogether. Elite athletes have been shown to decline by 43% from ages 23 to 50 (from 70 ml/kg/min to 40 ml/kg/min) when they stop training after their careers are over (24). In some cases, the relative decline is greater than for the average population - as much as 15% per decade or 1.5% per year (27,28).
However in comparison, master athletes who continue to keep fit only show a decrease of 5-6% per decade or 0.5-0.6% per year (25,26,27,28). When they maintain the same relative intensity of training, a decrease of only 3.6% over 25 years has been reported (28) and most of that was attributable to a small increase in bodyweight.
It seems that training can slow the rate of decline in VO2 max but becomes less effective after the age of about 50 (3).
References
1) Baechle TR and Earle RW. (2000) Essentials of Strength Training and Conditioning: 2nd Edition. Champaign, IL: Human Kinetics
2) McArdle WD, Katch FI and Katch VL. (2000) Essentials of Exercise Physiology: 2nd Edition Philadelphia, PA: Lippincott Williams & Wilkins
3) Wilmore JH and Costill DL. (2005) Physiology of Sport and Exercise: 3rd Edition. Champaign, IL: Human Kinetics
4) Sjodin B, Svedenhag J. Oxygen uptake during running as related to body mass in circumpubertal boys: a longitudinal study. Eur J Appl Physiol Occup Physiol. 1992;65(2):150-7
5) Costill DL. (1986) Inside Running: Basics of Sports Physiology. Indianapolis: Benchmark Press
6) Pollock ML. (1973). Quantification of endurance training programs. Exercise and Sport Sciences Reviews. 1,155-188
7) Saltin B, Rowell LB. Functional adaptations to physical activity and inactivity. Federation Proceeding. 1980 Apr;39(5):1506-13
8) Gollnick PD, Armstrong RB, Saubert CW 4th, Piehl K, Saltin B. Enzyme activity and fiber composition in skeletal muscle of untrained and trained men. J Appl Physiol. 1972 Sep;33(3):312-9
9) Saltin B, Nazar K, Costill DL, Stein E, Jansson E, Essen B, Gollnick D. The nature of the training response; peripheral and central adaptations of one-legged exercise. Acta Physiol Scand. 1976 Mar;96(3):289-305
10) Costill DL, Thomas R, Robergs RA, Pascoe D, Lambert C, Barr S, Fink WJ. Adaptations to swimming training: influence of training volume. Med Sci Sports Exerc. 1991 Mar;23(3):371-7
11) Bouchard C, Dionne FT, Simoneau JA, Boulay MR. Genetics of aerobic and anaerobic performances. Exerc Sport Sci Rev. 1992;20:27-58
12) Pollock ML, Foster C, Knapp D, Rod JL, Schmidt DH. Effect of age and training on aerobic capacity and body composition of master athletes. J Appl Physiol. 1987 Feb;62(2):725-31
13) Bouchard C, Shephard RJ, Stephens T, Sutton JR and McPherson BD (Eds.), Exercise Fitness and Health (pp. 147-153). Champaign, IL: Human Kinetics
14) Green HJ, Jones S, Ball-Burnett M, Farrance B, Ranney D. Adaptations in muscle metabolism to prolonged voluntary exercise and training. J Appl Physiol. 1995 Jan;78(1):138-45
15) Energetics in marathon running. Medicine and Science in Sports. 1969 1(2):81-86
16) Astrand P-O and Rodahl K. (1986) The Textbook of Work Physiology: Physiological Bases of Exercise (3rd ed.). New York: McGraw-Hill
17) Kraemer WJ, Deschenes MR, Fleck SJ. Physiological adaptations to resistance exercise. Implications for athletic conditioning. Sports Med. 1988 Oct;6(4):246-56
18) Hickson RC, Foster C, Pollock ML, Galassi TM, Rich S. Reduced training intensities and loss of aerobic power, endurance, and cardiac growth. J Appl Physiol. 1985 Feb;58(2):492-9
19) Costill DL, King DS, Thomas R and Hargreaves M. Effects of reduced training on muscular power in swimmers. Physician and Sports Medicine. 1985; 13(2), 94-101
20) Houmard JA, Costill DL, Mitchell JB, Park SH, Hickner RC, Roemmich JN. Reduced training maintains performance in distance runners. Int J Sports Med. 1990 Feb;11(1):46-52
21) Houmard JA, Scott BK, Justice CL, Chenier TC. The effects of taper on performance in distance runners. Med Sci Sports Exerc. 1994 May;26(5):624-31
22) Jackson AS, Beard EF, Wier LT, Ross RM, Stuteville JE, Blair SN. Changes in aerobic power of men, ages 25-70 yr. Med Sci Sports Exerc. 1995 Jan;27(1):113-20
23) Jackson AS, Wier LT, Ayers GW, Beard EF, Stuteville JE, Blair SN. Changes in aerobic power of women, ages 20-64 yr. Med Sci Sports Exerc. 1996 Jul;28(7):884-91
24) Dill DB, Robinson S, Ross JC. A longitudinal study of 16 champion runners. J Sports Med Phys Fitness. 1967 Mar;7(1):4-27
25) Hagerman FC, Fielding RA, Fiatarone MA, Gault JA, Kirkendall DT, Ragg KE, Evans WJ. A 20-yr longitudinal study of Olympic oarsmen. Med Sci Sports Exerc. 1996 Sep;28(9):1150-6
26) Pollock ML, Mengelkoch LJ, Graves JE, Lowenthal DT, Limacher MC, Foster C, Wilmore JH. Twenty-year follow-up of aerobic power and body composition of older track athletes. J Appl Physiol. 1997 May;82(5):1508-16
27) Trappe SW, Costill DL, Goodpaster BH, Pearson DR. Calf muscle strength in former elite distance runners. Scand J Med Sci Sports. 1996 Aug;6(4):205-10
28) Trappe SW, Costill DL, Vukovich MD, Jones J, Melham T. Aging among elite distance runners: a 22-yr longitudinal study. J Appl Physiol. 1996 Jan;80(1):285-90
29) Cureton KJ, Sparling PB. Distance running performance and metabolic responses to running in men and women with excess weight experimentally equated. Med Sci Sports Exerc. 1980;12(4):288-94
30) Dudley GA, Fleck SJ. Strength and endurance training. Are they mutually exclusive? Sports Med. 1987 Mar-Apr;4(2):79-85
31) Fleck SJ. Cardiovascular adaptations to resistance training. Med Sci Sports Exerc. 1988 Oct;20(5 Suppl):S146-51
32) Kraemer WJ, Duncan ND, Volek JS. Resistance training and elite athletes: adaptations and program considerations. J Orthop Sports Phys Ther. 1998 Aug;28(2):110-9
33) Kraemer WJ, Patton JF, Gordon SE, Harman EA, Deschenes MR, Reynolds K, Newton RU, Triplett NT, Dziados JE. Compatibility of high-intensity strength and endurance training on hormonal and skeletal muscle adaptations. J Appl Physiol. 1995 Mar;78(3):976-89
1) Baechle TR and Earle RW. (2000) Essentials of Strength Training and Conditioning: 2nd Edition. Champaign, IL: Human Kinetics
2) McArdle WD, Katch FI and Katch VL. (2000) Essentials of Exercise Physiology: 2nd Edition Philadelphia, PA: Lippincott Williams & Wilkins
3) Wilmore JH and Costill DL. (2005) Physiology of Sport and Exercise: 3rd Edition. Champaign, IL: Human Kinetics
4) Sjodin B, Svedenhag J. Oxygen uptake during running as related to body mass in circumpubertal boys: a longitudinal study. Eur J Appl Physiol Occup Physiol. 1992;65(2):150-7
5) Costill DL. (1986) Inside Running: Basics of Sports Physiology. Indianapolis: Benchmark Press
6) Pollock ML. (1973). Quantification of endurance training programs. Exercise and Sport Sciences Reviews. 1,155-188
7) Saltin B, Rowell LB. Functional adaptations to physical activity and inactivity. Federation Proceeding. 1980 Apr;39(5):1506-13
8) Gollnick PD, Armstrong RB, Saubert CW 4th, Piehl K, Saltin B. Enzyme activity and fiber composition in skeletal muscle of untrained and trained men. J Appl Physiol. 1972 Sep;33(3):312-9
9) Saltin B, Nazar K, Costill DL, Stein E, Jansson E, Essen B, Gollnick D. The nature of the training response; peripheral and central adaptations of one-legged exercise. Acta Physiol Scand. 1976 Mar;96(3):289-305
10) Costill DL, Thomas R, Robergs RA, Pascoe D, Lambert C, Barr S, Fink WJ. Adaptations to swimming training: influence of training volume. Med Sci Sports Exerc. 1991 Mar;23(3):371-7
11) Bouchard C, Dionne FT, Simoneau JA, Boulay MR. Genetics of aerobic and anaerobic performances. Exerc Sport Sci Rev. 1992;20:27-58
12) Pollock ML, Foster C, Knapp D, Rod JL, Schmidt DH. Effect of age and training on aerobic capacity and body composition of master athletes. J Appl Physiol. 1987 Feb;62(2):725-31
13) Bouchard C, Shephard RJ, Stephens T, Sutton JR and McPherson BD (Eds.), Exercise Fitness and Health (pp. 147-153). Champaign, IL: Human Kinetics
14) Green HJ, Jones S, Ball-Burnett M, Farrance B, Ranney D. Adaptations in muscle metabolism to prolonged voluntary exercise and training. J Appl Physiol. 1995 Jan;78(1):138-45
15) Energetics in marathon running. Medicine and Science in Sports. 1969 1(2):81-86
16) Astrand P-O and Rodahl K. (1986) The Textbook of Work Physiology: Physiological Bases of Exercise (3rd ed.). New York: McGraw-Hill
17) Kraemer WJ, Deschenes MR, Fleck SJ. Physiological adaptations to resistance exercise. Implications for athletic conditioning. Sports Med. 1988 Oct;6(4):246-56
18) Hickson RC, Foster C, Pollock ML, Galassi TM, Rich S. Reduced training intensities and loss of aerobic power, endurance, and cardiac growth. J Appl Physiol. 1985 Feb;58(2):492-9
19) Costill DL, King DS, Thomas R and Hargreaves M. Effects of reduced training on muscular power in swimmers. Physician and Sports Medicine. 1985; 13(2), 94-101
20) Houmard JA, Costill DL, Mitchell JB, Park SH, Hickner RC, Roemmich JN. Reduced training maintains performance in distance runners. Int J Sports Med. 1990 Feb;11(1):46-52
21) Houmard JA, Scott BK, Justice CL, Chenier TC. The effects of taper on performance in distance runners. Med Sci Sports Exerc. 1994 May;26(5):624-31
22) Jackson AS, Beard EF, Wier LT, Ross RM, Stuteville JE, Blair SN. Changes in aerobic power of men, ages 25-70 yr. Med Sci Sports Exerc. 1995 Jan;27(1):113-20
23) Jackson AS, Wier LT, Ayers GW, Beard EF, Stuteville JE, Blair SN. Changes in aerobic power of women, ages 20-64 yr. Med Sci Sports Exerc. 1996 Jul;28(7):884-91
24) Dill DB, Robinson S, Ross JC. A longitudinal study of 16 champion runners. J Sports Med Phys Fitness. 1967 Mar;7(1):4-27
25) Hagerman FC, Fielding RA, Fiatarone MA, Gault JA, Kirkendall DT, Ragg KE, Evans WJ. A 20-yr longitudinal study of Olympic oarsmen. Med Sci Sports Exerc. 1996 Sep;28(9):1150-6
26) Pollock ML, Mengelkoch LJ, Graves JE, Lowenthal DT, Limacher MC, Foster C, Wilmore JH. Twenty-year follow-up of aerobic power and body composition of older track athletes. J Appl Physiol. 1997 May;82(5):1508-16
27) Trappe SW, Costill DL, Goodpaster BH, Pearson DR. Calf muscle strength in former elite distance runners. Scand J Med Sci Sports. 1996 Aug;6(4):205-10
28) Trappe SW, Costill DL, Vukovich MD, Jones J, Melham T. Aging among elite distance runners: a 22-yr longitudinal study. J Appl Physiol. 1996 Jan;80(1):285-90
29) Cureton KJ, Sparling PB. Distance running performance and metabolic responses to running in men and women with excess weight experimentally equated. Med Sci Sports Exerc. 1980;12(4):288-94
30) Dudley GA, Fleck SJ. Strength and endurance training. Are they mutually exclusive? Sports Med. 1987 Mar-Apr;4(2):79-85
31) Fleck SJ. Cardiovascular adaptations to resistance training. Med Sci Sports Exerc. 1988 Oct;20(5 Suppl):S146-51
32) Kraemer WJ, Duncan ND, Volek JS. Resistance training and elite athletes: adaptations and program considerations. J Orthop Sports Phys Ther. 1998 Aug;28(2):110-9
33) Kraemer WJ, Patton JF, Gordon SE, Harman EA, Deschenes MR, Reynolds K, Newton RU, Triplett NT, Dziados JE. Compatibility of high-intensity strength and endurance training on hormonal and skeletal muscle adaptations. J Appl Physiol. 1995 Mar;78(3):976-89
http://www.sport-fitness-advisor.com/VO2max.html
No comments:
Post a Comment